Mean Arterial Pressure
Mean Arterial Pressure (MAP) = CO x Systemic Vascular Resistance (SVR)
Therefore in states of low CO or reduced SVR (e.g. sepsis, anaesthesia) then the MAP will be lower.
MAP is often the target set for blood pressure in ICU. It is thought that organ bloodflow depends on MAP as opposed to a systolic blood pressure.
Some caveats to this include:
- Diastolic pressure is the pressure that perfuses the coronary arteries
- Systolic blood pressure is important in the management of certain patients (e.g. acute aortic syndromes, ICH)
Indications
Generic reasons for insertion are:
- Need for invasive haemodynamic monitoring (e.g. on vasopressors) or
- Need for frequent arterial blood sampling.
Complications
- Thrombosis or stricture formation
- Infection
- Haematoma
- Inadvertent arterial drug administration
- Pseudo-aneurysm
- Dissection
- A-V fistula.
Insertion sites
Most commonly placed in radial or femoral arteries. Other sites of insertion include brachial artery (this is an end artery so the consequence of thrombosis can be catastrophic to a patient) or dorsalis pedis.
Equipment for insertion
- Arterial cannula – using a kit with separate needle and guidewire can be easier to manipulate and reposition if needed.
- The remainder of equipment needed includes pressure bag and fluid, transducer, 3 way tap and 1.2m of non-compressible tubing to connect the pressure bag to the cannula.
Troubleshooting
Why does my non-invasive blood pressure differ to my arterial BP?
Calibration
- “Zero-ing” – important to ensure transducer zeroed. This ensures that the transducer references atmospheric pressure as zero.
- Transducer height (levelling) – needs to be at level of right atrium (phlebostatic axis). For every 10cm below the phlebostatic axis the transducer will add 7.4mmHg of pressure and vice versa.
Damping
Diagnosing a problem with damping
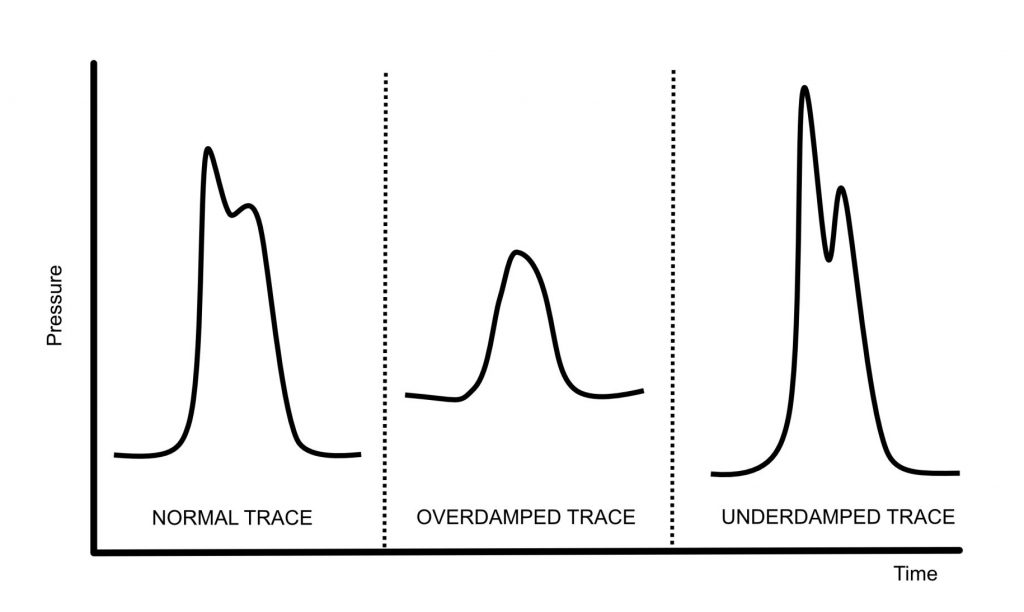
Look at the arterial line’s trace:
- Overdamped
- Fine detail lost and trace looks flat
- Underestimates SBP, overestimated DBP, MAP usually accurate
- On square wave test – no oscillations
- Underdamped
- Lots of artefacts present
- Overestimated SBP, underestimated DBP, MAP usually accurate
- On square wave test – multiple oscillations
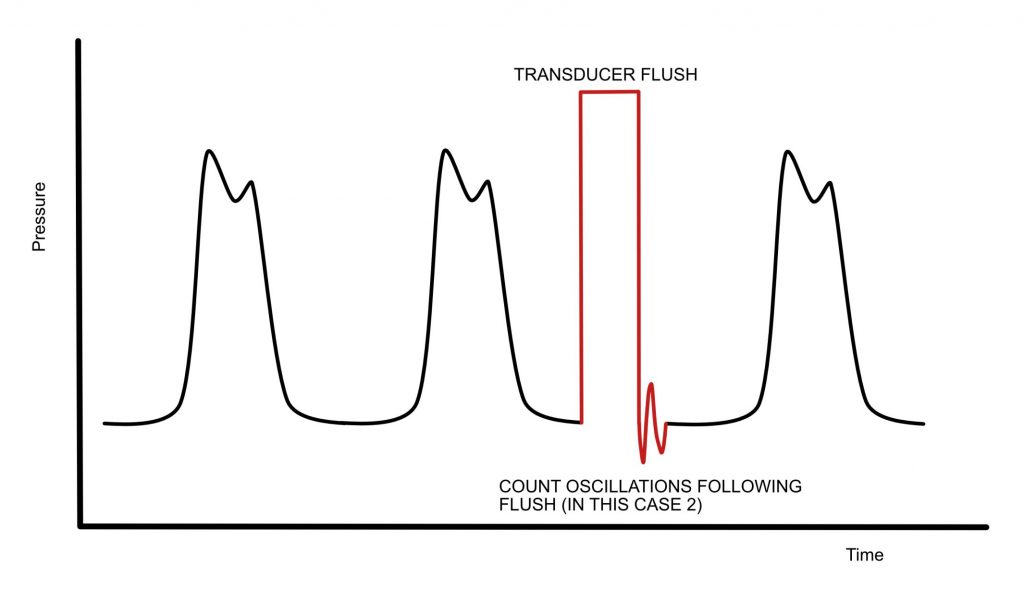
Perform the square-wave or fast-flush test:
- System is flushed.
- A correctly damped arterial line should have 2 oscillations following the flush and then return to its baseline.
Fixing an over-damped or under-damped trace
- If you notice an overdamped or underdamped trace, then ensure:
- the catheter is not kinked
- the pressure bag pressurised to 300mmHg
- there are no bubbles or clots visible in the line
- You can try flushing the line but often after a period of time the arterial waveform will be inaccurate and you may not be able to aspirate from the arterial cannula. This may require a new arterial line to be sited.
Arterial Lines: How to….
Below is an excellent video by Cassie Roberts and the Eastern Health ICU Education team that explain some of the practicalities and skills in setting up and using an arterial lines. These are skills we should all be able to do when it comes to helping manage the critically ill.
References and Further Reading
Core EM: How to set up an arterial line
Taming the SRU: Arterial Line Placement
Author: George Walker