The key events in normal neuromuscular transmission are:
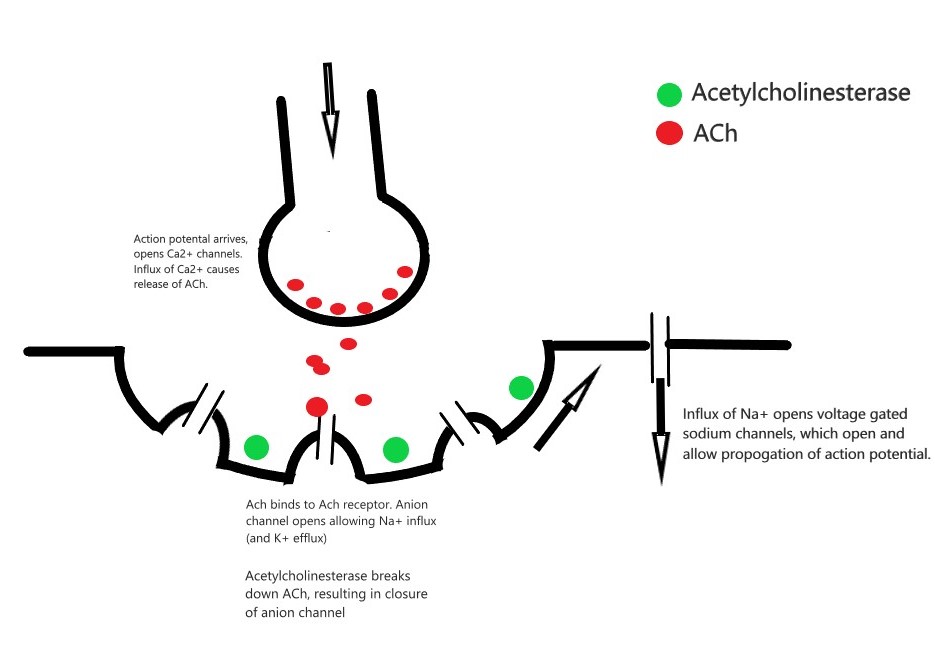
- The arrival of an action potential causes release of acetylcholine (ACh), a neurotransmitter, from the pre-synaptic membrane.
- ACh binds with nicotinic receptors on the post-synaptic membrane resulting in the opening of an anion channel in the motor end plate.
- The open anion channels allow Na+ influx (and K+ efflux). This causes a voltage change across the membrane and the development of an end plate potential.
- The end plate potential opens voltage gated sodium channels, allowing further Na+ influx. This depolarises the membrane and generates an action potential that can propagate further along the muscle fibre.
- Acetylcholinesterase breaks down ACh, resulting in closure of the anion channels and voltage gated sodium channels.
- Extra-junctional ACh receptors can proliferate markedly as part of body’s response to injury (burns, paraplegia) or in neuromuscular disorders. The significantly increased number of receptors can severely increase the amount of potassium that leaks out of the muscle fibres when open, leading to fatal hyperkalaemia.
Common uses of neuromuscular blockade include endotracheal intubation, and patient-ventilator dysynchrony. Neuromuscular blockers can be split into depolarising (e.g. Suxamethonium) and non-depolarising drugs (e.g. Rocuronium and Cisatracurium)
- Suxamethonium
- Structurally two joined ACh groups which bind to the post-synaptic ACh receptor and causes depolarisation. Suxamethonium cannot be broken down by acetylcholinesterase. Therefore, remains bound to the receptor and the ACh receptor is unable to repolarise. Until repolarisation occurs, any subsequent binding of ACh has no effect, resulting in muscle paralysis.
- Dosing: 1-2mg/kg. Onset in 30-60 seconds, lasts 2-3 minutes.
- Metabolised by plasma pseudocholinesterases.
- Side Effects:
- CVS: Bradycardia
- RESP: Suxamethonium Apnoea – prolonged duration of effect due to congenital or acquired abnormalities of pseudocholinesterases that cannot break down suxamethonium
- CNS: Increased intra-gastric, intra-ocular and intra-cranial pressures
- RENAL: Hyperkalaemia (can be fatal in burns patients, paraplegics and neuromuscular disorders) due to K+ efflux.
- METABOLIC: Malignant hyperthermia
- MSK: Myalgia
- IMMUNE: Anaphylaxis
- Rocuronium
- Competitively antagonises (“blocks”) ACh receptors and therefore prevents ACh binding and exerting its normal effect.
- Dosing: 0.6 – 1.2mg/kg. 1.2mg/kg provides faster onset (typically 60-90 seconds), lasts 30-45 minutes
- Eliminated in bile and urine
- Side Effects:
- CVS: Tachycardia
- IMMUNE: Anaphylaxis
- MSK: Critical illness myopathy with long term use
- Reversal:
- Suggamadex – forms a complex with rocuronium which has no biological action. Dose following RSI is 16 mg/kg.
- Cistracurium
- Often given as an infusion due to Hoffman elimination (an organ independent method of metabolism) that will result in quick cessation of effect when infusion ceased.
- Minimal risk of anaphylaxis
Author: George Walker